
Bladder cancer
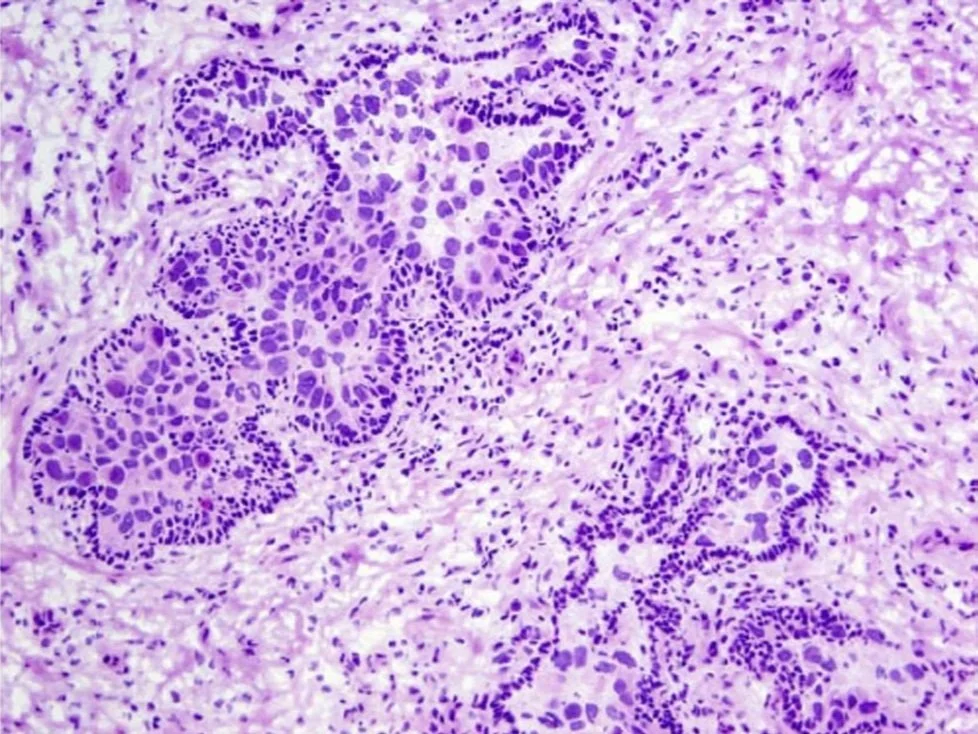
Also known as urothelial carcinoma, transitional cell carcinoma, and depending on depth of invasion, non-muscle invasive bladder cancer and muscle invasive bladder cancer
Dr. Ned Kinnear
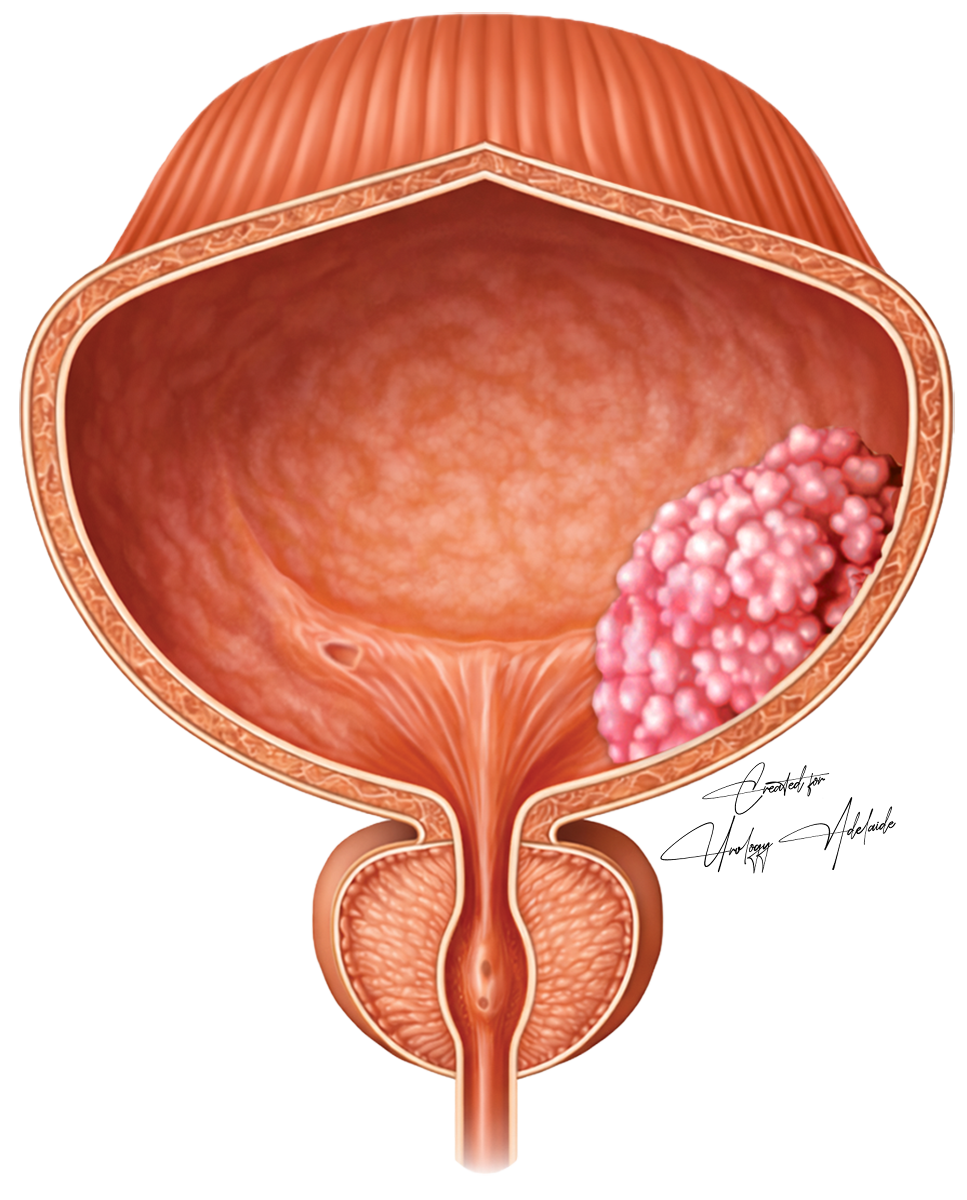
Bladder cancer: an overview
Bladder cancer is uncommon
While relatively uncommon, bladder cancer can be lethal
Approximately 1,000 Australians die from this disease each year
There are many ways to treat bladder cancer
Flexible cystoscopy: a flexible camera to look inside the bladder, can be performed under general or local anaesthesia
Rigid cystoscopy + biopsy: a stiff camera to examine the inside of a bladder, and take small specimens to assessment under the microscope. This is only done under general anaesthesia.
Trans urethral resection of bladder tumour (TURBT) +/- instilling chemotherapy into the bladder



Three stages of bladder cancer
Bladder cancer have different stages of aggressiveness and spread. Each will have varying treatment options.
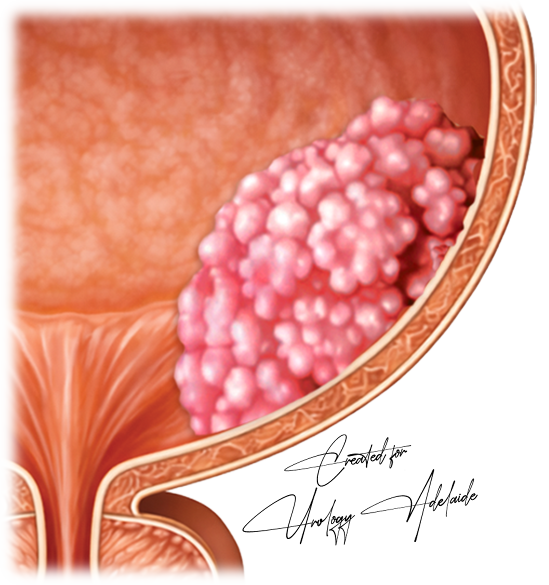
NMIBC
Non-muscle invasive bladder cancer
The tumour is limited to the inner two layers of the bladder (urothelium and lamina propria).
Within NMIBC, a patient may be further classified as low, intermediate, high or very high risk (of tumour progressing deeper into the bladder wall layers)
This classification is based the number of bladder tumours present and their size, grade (degree of cell abnormality), stage (depth of invasion), presence of carcinoma in-situ (a high risk non-invasive flat tumour), as well as the patient’s age and gender.
Treatment commences with tumour resection (TURBT)
Treatment can subsequently include observation (with regular camera checks into the bladder), liquid intravesical (into the bladder) treatments such as immunotherapy (Bacillus Calmette-Guérin; BCG) or chemotherapy (mitomycin, epirubicin, gemcitabine) or radical cystectomy (removal of the entire bladder).
MIBC
Muscle invasive bladder cancer
The tumour invades the muscle layer (muscularis propria)
This is life-threatening
The chief treatment options are radical cystectomy (removal of the entire bladder) often paired with chemo-therapy beforehand, or repeat TURBT paired with chemotherapy and radiotherapy.
mUC (U stands for urothelial)
Metastatic bladder cancer
The tumour has spread to other organs.
Your urologist will manage your condition in association with medical oncologists and other specialists.
Treatments can include radiotherapy and intravenous (into the veins) chemotherapy and/ or immunotherapy.
The focus moves from disease cure to disease control and symptom management.