
Prostate cancer
“Most men diagnosed with prostate cancer do not die from it, and live long, active, happy lives”
Dr. Ned Kinnear
Prostate cancer: an overview
Prostate cancer is common
Each year, 30,000 Australian men are diagnosed with prostate
By age 85, 1 in 5 men will be diagnosed with prostate cancer.
However, there is much good news
Most men with prostate cancer do not die from prostate cancer.
Most prostate cancers present at an early stage (localised).
Across all stages of prostate cancer, management has improved dramatically
For men with localised low-risk prostate cancer, active surveillance is the most common management.
Intervention (and its side effects) is initially deferred, while the patient’s prostate is closely monitored.
For men with localised intermediate- or high-risk prostate cancer, surgery or radiotherapy are the main two treatment options. Both are substantially more sophisticated compared to 20 years ago, with reduced side effects.
For men with prostate cancer that has spread (metastatic), treatment has also dramatically improved.
I have localised prostate cancer. Now what?

Helpful ways of thinking about prostate cancer, next steps, and key things to keep in mind when deciding what is the right option for you. Dr. Kinnear recommends three main focuses.
The first focus
Understanding your specific prostate cancer
The first thing to do is understand your cancer’s stage and grade. This is done by performing three to four tests, some of which you may have already had. They include:
Prostate-specific antigen (PSA) blood test
Magnetic resonance imaging (MRI) scan of the prostate
Transperineal prostate biopsy procedure
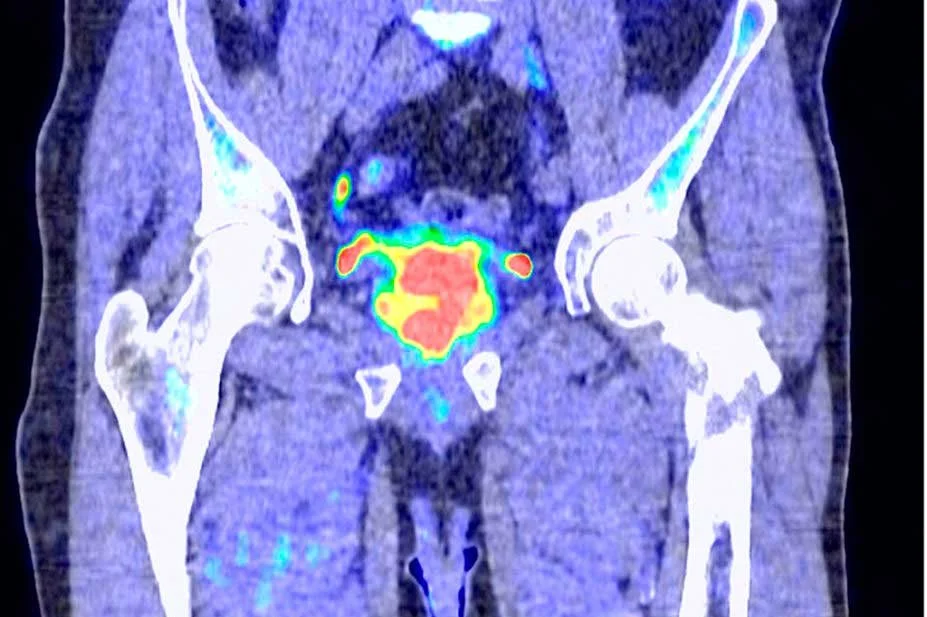
Most patients also require staging imaging such as PSMA PET scan
The second focus
Well-informed decisions
The second focus is to make a well-informed decision, with strong support from your loved ones. The diagnosis of cancer is often a time of huge anxiety and disorientation. Although it can be normal to feel the desire to ‘get 'on’, make a decision and start treatment, most prostate cancer moves very slowly.
There is time (up to three months) to gain broad perspectives, through speaking with your family, general practitioner and others.
The third focus
Having the right team
Choosing the best team to look after you on your prostate cancer journey is important. Factors you could consider include surgeon’s expertise, fellowship training, costs, location, availability, and how you connect with the surgeon. A patient’s relationship with urologists are often longitudinal as there are periods of follow up after the surgery.
Dr. Ned Kinnear prioritises being a skilled surgeon with two fellowships, one of which is focused on minimally-invasive robotic surgery. Ned also focuses ensuring that you have a comprehensive understanding of your prostate cancer, and guiding you to the right treatment during what can be a stressful time.
What are the stages of prostate cancer?
How we measure and quantify where the prostate cancer is
Your urologist often uses MRI and PSMA PET scans to help them understand where your prostate cancer is.
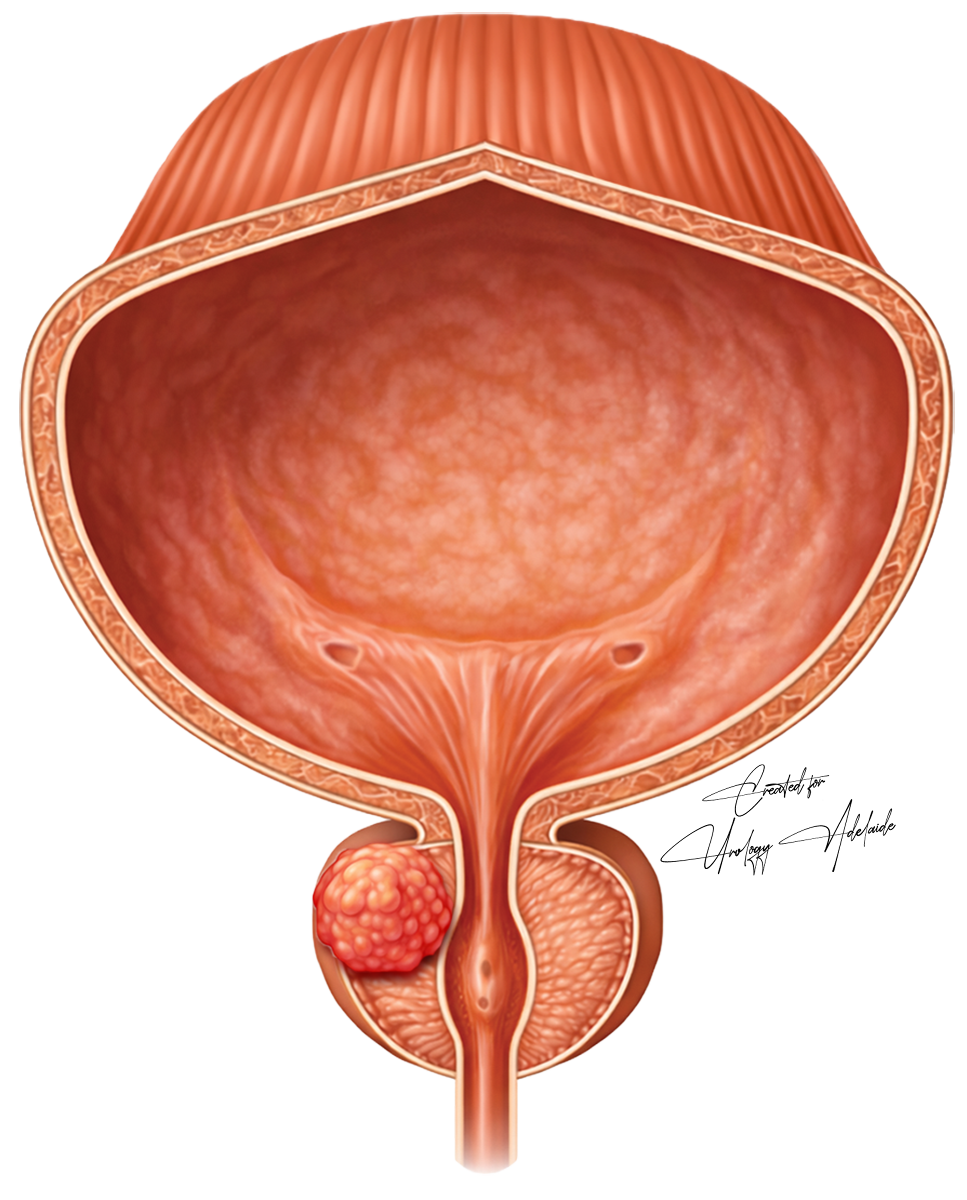
Localised the cancer exists completely in the prostate
Locally advanced the cancer has grown a little into nearby fat, or the seminal vesicles (glands behind the prostate)
Metastatic the cancer has spread further, to lymph nodes, bone or other organs. The focus of metastatic prostate moves from cure to control.
Treatment options for localised prostate cancer



-
This is an option for men with low-risk disease, as well as select men with intermediate-risk disease. Men are watched closely with regular examinations, blood tests (PSA) and scans.
Dr. Kinnear deliver evidence-based care, and follow the PRIAS protocol for active surveillance.
Pros: men defer treatment and its side effects, typically for several years.
Cons: in approximately 1% of patients, the prostate cancer will spread (metastasise) during surveillance and the patient will lose their window for cure.
-
The prostate gland is surgically removed.
The patient is asleep and typically goes home the following day. Dr. Kinnear uses the advanced Da Vinci Xi robotic surgery platform to perform robotic-assisted radical prostatectomy (RARP). Dr Kinnear specialises in robotic surgery.
Pros: approximately 80% of patient are cured. Treatment is completed with a single visit. There is no risk of radiation damage to the bladder, rectum (back passage) or urethra (urine tube).
Cons: >50% of men will develop erectile dysfunction, and 5-10% will develop bothersome urinary incontinence. Other possible complications include heart or lung events, bleeding or rectal injury. Some patients are not candidates for surgery. -
High-energy radiation is directed at the prostate, either with external beams or with seeds or rods placed directly into the gland. Radiotherapy is delivered by specialists known as radiation oncologists.
Pros: Same high cure rate as surgery. The patient avoids some of the risks of surgery. Most patients are eligible for radiotherapy.
Cons
Approximately 38 hospital attendances are required for the course of treatment. Most men also receive adjuvant hormonal therapy (ADT), which has many possible side effects.
Following radiation, >50% of men will develop erectile dysfunction, and 3% will develop bothersome urinary incontinence.
10% of men will develop radiation-induced damage. Radiation-induced damage is incurable and can significantly impact quality of life. Possible affected organs include:
Bladder, causing bleeding or overactive bladder,
Rectum (back passage), causing bleeding, faecal urgency or faecal incontinence)
Urethra (urine pipe), causing a stricture (narrowing).